
This is one of the most common tutorial topics. Why? Because there’s so much to know, it’s a common reason for women consulting, and it’s something that we don’t spend much time thinking about during our hospital jobs – even Obstetrics and Gynaecology posts!
It’s daunting because there are so many options, and so many situations. Who can have what, and when? What are the side effects? How should it be used?
I am not going to talk about all the methods in-depth here. I thought I would start with a quick overview of the options available, and a fact or two about each to get us started. My knowledge is derived from the Faculty of Sexual and Reproductive Healthcare (FSRH) guidance and the online learning modules that comprise the DFSRH.
One thing I like to do when learning is relate clinical knowledge back to anatomy and physiology. I find that by doing this, things just make sense, and tend to stick in my mind better. So you might notice that this post relates back to the physiology of the menstrual cycle!
So what’s available?
Barrier Methods:
- Male or female condoms
- Diaphragms
- Caps
I’m not going to discuss barrier methods any further!
Combined Hormonal Contraception (CHC):
- Pills
- Patch
- Ring
Progesterone only methods:
- Pills
- Injection
- Implant
- IUS
Non- hormonal:
- Copper IUD
You can see why it’s so confusing for both the patient, and the doctor! Within these methods – there are so many brands!
But who are the main players, where hormones are concerned, in the reproductive cycle?
Well we need FSH and LH release from the pituitary gland. These hormones are working on the ovaries to ensure maturation of oocytes occurs over the cycle, and to facilitate the release of one each month. As this is occurring there are changes occurring within the uterus to prepare for potential implantation, and subsequent pregnancy.
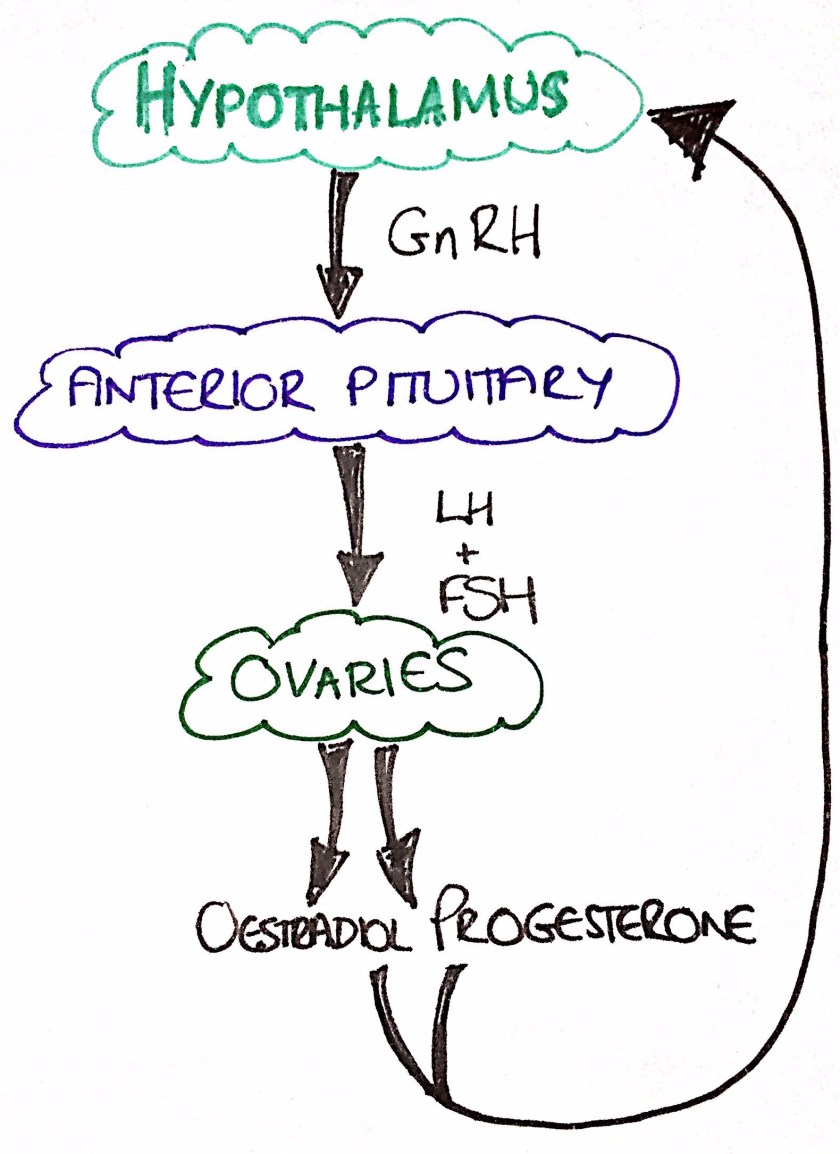
Why is it useful to know this physiology? Because it lets us work out how the different contraceptions might be working to prevent pregnancy, and how they may impact upon the woman’s bleeding patterns.

Thus, progesterone within combined hormonal contraception (CHC) impacts upon the feedback cycle of these hormones to eventually prevent the mid-cycle LH surge, along with it’s affects on cervical mucus. Oestrogen within CHC is acting upon the endometrium, and preventing follicular development.
Progesterone only methods are slightly more complex, because it depends a little on the specific progesterone, and how it’s given, as to how exactly it affects the cycle:
- The injection suppresses ovulation
- The progesterone only pill’s (POP) main action is via effects on cervical mucus, but may or may not suppress ovulation (desogestrel, found in brands such as Cerazette and Cerelle, suppresses ovulation in approximately 97% of cycles)
- The implant often suppresses ovulation but this is not absolute, and certainly not towards the end of the 3 years.
- Progesterone emergency contraception prevents the LH surge thus arresting follicular development and delaying ovulation
- The IUS (e.g. Mirena) has it’s greatest effects on the endometrium and thickening of cervical mucus. It inhibits proliferation of the endometrium, thus making it thin and atrophic.
The Copper IUD, as a non-hormonal method, works by producing a foreign body reaction. It can also affect endometrial enzymes, and copper has a direct toxic effect on sperm and ova. It’s primary mechanism of action is the prevention of fertilisation. However, it can be used as an emergency contraception to prevent implantation.
With perfect use, all methods of hormonal contraception are very effective at preventing pregnancy. However, methods that require patient action (pills and the injection) tend to have higher pregnancy rates, and greater discrepancy in typical versus perfect use. The most effective method at preventing pregnancy is the implant. The Mirena IUS and the implant have a greater impact upon pregnancy prevention that female sterilisation.
That was an initial introduction to contraception. It gives you an idea of whats out there, how they work and how they link into the physiology of the menstrual cycle.
There is much more to know, in order to allow women to make informed choices, and help us consider what might be right, and safe, for the woman.
Let me know if you have any thoughts on the above – and through your comments give me an idea of where we should move on to next within the subject of contraception.
